Translational medicine is defined as the systematic process of converting laboratory discoveries into clinical therapies by aligning preclinical evidence, clinical trial design, and real-world outcomes within a single, decision-driven pipeline. The role of translational medicine in biotech is not peripheral. It is the operational core that determines whether a promising compound reaches patients or dies in a filing cabinet. NCATS at NIH exists precisely to remove the bottlenecks that kill otherwise viable therapies, using better patient-response models, enhanced clinical trial design, and real-world data integration. For biotechnology professionals, understanding how translational medicine functions across the full development arc is the difference between efficient pipelines and expensive late-stage failures.
What is the role of translational medicine in biotech pipelines?
Translational medicine in biotech operates as the connective tissue between discovery science and clinical proof of concept. It is not a single department or a phase of development. It is a design philosophy applied from the first experiment to post-market evidence generation.

The standard industry term for this practice is "bench-to-bedside translation," though the field has expanded well beyond that linear metaphor. Modern translational medicine strategies now include bedside-to-bench feedback loops, where clinical observations inform new mechanistic hypotheses. This bidirectional flow is what separates a mature translational program from a traditional sequential drug development model.
The impact of biotechnology on this process has been transformative. Biotech companies, unlike large pharmaceutical firms, often operate with lean teams and compressed timelines. Translational medicine gives those teams a structured framework for making go/no-go decisions with confidence, even under resource constraints. The result is faster identification of compounds worth advancing and earlier termination of those that will fail.
Three foundational elements define a functional translational medicine program in biotech:
- Biomarker integration: Validated biomarkers link preclinical pharmacodynamic signals to measurable clinical endpoints, reducing ambiguity at every decision gate.
- Mechanistic alignment: The mechanism of action studied in animal models must map directly to the human pathology being targeted, not just produce a phenotypic response.
- Regulatory anticipation: Every dataset generated should be pre-assigned a role in the eventual IND submission or clinical protocol, not collected speculatively.
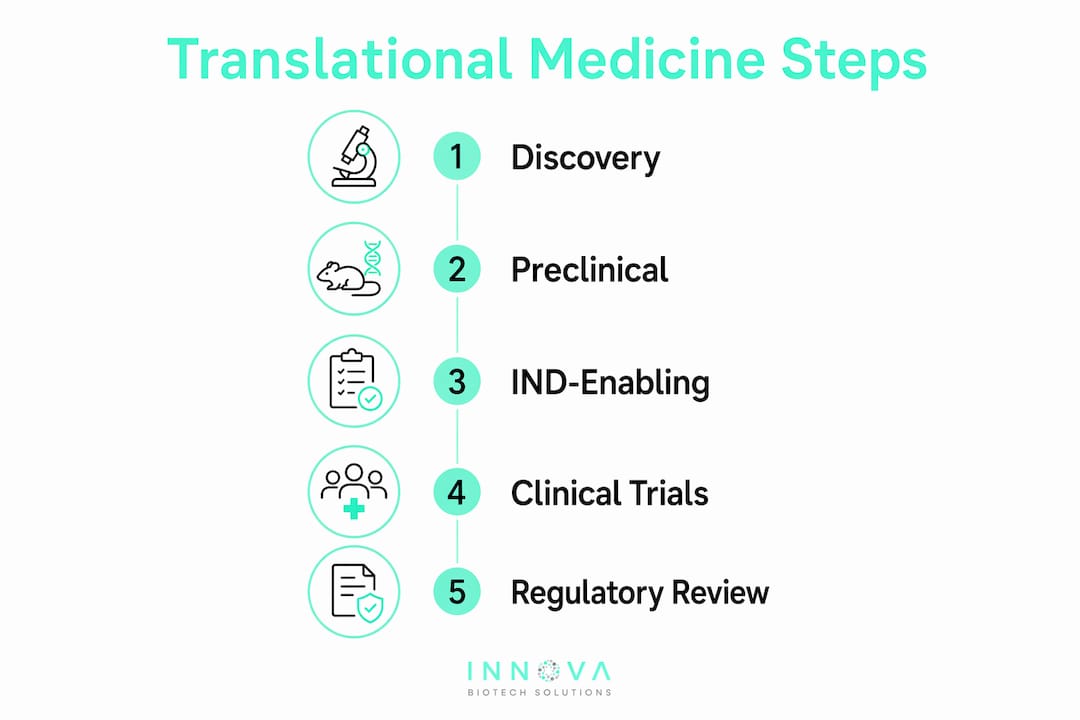
How does preclinical study design inform clinical development?
Translational preclinical research treats each dataset as a link in an evidence chain, pre-assigned to answer a specific regulatory or clinical question before the first animal is enrolled. This discipline eliminates the common failure mode of generating abundant data that cannot answer the question regulators actually ask.
IND-enabling studies are the clearest expression of this principle. Dose selection for first-in-human trials requires cross-species pharmacokinetic and pharmacodynamic modeling, GLP-compliant toxicology, and safety biomarker identification that will translate to clinical monitoring. ICH guidelines, particularly ICH M3(R2) and ICH S9, define the minimum evidence package. Translational medicine strategies add a layer above compliance: they ask whether the data package is sufficient to make a confident clinical decision, not just a permissible one.
Biomarker validation across species is where many biotech programs underinvest. A biomarker that predicts response in a mouse xenograft model has limited value unless its human analog is measurable in accessible tissue, correlates with clinical outcomes in prior studies, and can be standardized across clinical sites. Translational medicine demands this validation work happen before Phase I, not during it.
Pro Tip: When designing IND-enabling studies, map each assay to a specific clinical question in a translational evidence matrix. This document becomes the scientific rationale section of your IND and forces the team to identify evidence gaps before they become regulatory deficiencies.
The structured decision gates that define translational preclinical programs also discipline resource allocation. Teams that define explicit go/no-go criteria before generating data are less susceptible to confirmation bias and more likely to terminate non-viable programs before Phase II spending begins.
How does translational medical affairs improve regulatory and payer outcomes?
Translational Medical Affairs (TMA) is an emerging operating model that embeds Medical Affairs professionals into the development pipeline from preclinical stages onward, rather than activating them at launch. TMA coordinates preclinical, clinical, and real-world evidence generation to align clinical trial design with both regulatory requirements and payer evidence standards simultaneously.
The contrast with traditional Medical Affairs is significant. Conventional models deploy Medical Affairs after Phase III data is locked, at which point evidence gaps are expensive or impossible to close. TMA anticipates those gaps during study design, when adding a secondary endpoint or a patient-reported outcome measure costs almost nothing.
The practical benefits of early TMA embedding include:
- Payer evidence needs are identified during protocol design, not after submission.
- Clinical trial endpoints are validated for real-world relevance, not just regulatory acceptance.
- Publication strategy aligns with lifecycle evidence planning from the start.
- Regulatory feedback loops are shorter because Medical Affairs has maintained continuous dialogue with clinical teams.
"Embedding Medical Affairs early enhances payer positioning, reduces late-stage risk, and accelerates clinical adoption of new therapies." MedSurg PI, 2026
The feedback loop TMA creates runs in both directions. Post-market real-world evidence informs the next generation of clinical hypotheses, and those hypotheses feed back into preclinical mechanistic work. For biotech companies managing multiple pipeline assets, this continuous loop is a competitive advantage that compounds over time.
What advanced platforms are reshaping translational biotech research?
The translational medicine applications available to biotech teams in 2026 extend well beyond traditional cell and animal models. Three platform categories are producing measurable improvements in the predictive accuracy of preclinical work.
| Platform | Core capability | Translational value |
|---|---|---|
| Organs-on-chips | Human physiology modeling with biosensors | Quantitative benchmarking against clinical PK/tox data |
| AI and multi-omics | Target identification and trial optimization | Accelerated lead selection and precision patient stratification |
| TrialMatchAI | EHR-integrated patient-to-trial matching | Reduced recruitment heterogeneity and faster enrollment |
Organs-on-chips platforms provide reproducible human physiology models that benchmark quantitatively against clinical pharmacokinetics and toxicology data. Regulatory acceptance of these platforms is advancing, but it requires standardized measurement plans that link chip readouts directly to clinical data. Teams that invest in this documentation now will have a regulatory advantage as FDA and EMA guidance matures.
AI and multi-omics integration accelerates target identification, lead optimization, and precision clinical trial design. The challenge is not the technology. It is harmonizing diverse data streams, including genomics, proteomics, metabolomics, and clinical phenotyping, into reproducible, decision-ready outputs. Bench-to-clinic frameworks that standardize data ingestion and analysis pipelines are the prerequisite for realizing this value. For biotech teams working on target identification, multi-omics integration is now a baseline expectation, not an advanced capability.
TrialMatchAI uses explainable AI and standardized data formats to match patient biomarker and genetic profiles to clinical trial eligibility criteria through EHR integration. This directly addresses one of the most persistent failure modes in translational clinical research: enrolling heterogeneous patient populations that obscure treatment signals.
Pro Tip: Before adopting any organs-on-chip or AI platform, define the specific clinical question the platform must answer and the quantitative threshold that constitutes a valid result. Platforms adopted without fit-for-context specifications generate data that cannot be used in regulatory submissions.
How can biotech teams overcome the valley of death?
The "valley of death" describes the funding and infrastructure gap between academic discovery and clinic-ready product development. Universities fuel biotech innovation but consistently fail to bridge this gap because translational funding mechanisms and core facilities are underdeveloped relative to basic research infrastructure.
The consequences are concrete. A compound with validated mechanism and promising efficacy data can stall for years because no team has the resources or expertise to generate the IND-enabling package a venture investor or pharma partner requires. Good science is not enough. Translation must be designed from day one, with incentivized teams and defined milestones that create investable proof-of-concept packages.
Biotech companies bridging this gap successfully share several structural features:
- Translational core facilities or contracted CRO partnerships that provide GLP-compliant study execution without full internal infrastructure.
- Proof-of-concept funding mechanisms, including SBIR/STTR grants and academic-industry co-development agreements, that de-risk early translation.
- Cross-functional teams that include regulatory, clinical, and commercial expertise from the earliest stages, not just scientific leads.
- Coordinated ecosystem teamwork with a clear line of sight to patient impact, which prevents the isolated scientific excellence that produces publishable results but not developable products.
The valley of death is not primarily a scientific problem. It is an organizational and incentive design problem. Biotech teams that treat translation as a team sport, with shared accountability for clinical feasibility, consistently outperform those that treat it as a handoff between functions.
Practical strategies for implementing translational medicine in biotech
Biotech professionals integrating translational medicine approaches into their pipelines benefit from a structured implementation framework. The following sequence reflects current best practice across preclinical, clinical, and evidence-generation phases.
- Define decision gates before generating data. Every study should be designed around a specific go/no-go criterion. If the data cannot change a decision, the study should not be run.
- Standardize biomarkers across the development arc. Select biomarkers during target validation that are measurable in accessible human tissue and have prior clinical correlation data. Avoid species-specific surrogates that cannot translate.
- Embed Medical Affairs at IND stage. TMA involvement during protocol design costs nothing and prevents the evidence gaps that cost millions to address post-Phase III.
- Adopt fit-for-context translational platforms. Organs-on-chips, AI-driven multi-omics, and tools like TrialMatchAI each address specific translational bottlenecks. Select platforms based on the specific question they answer, not their novelty.
- Test clinical feasibility before committing to Phase II design. Patient availability, site capabilities, and biomarker assay logistics should be validated before the protocol is finalized. Late-stage feasibility failures are among the most expensive in drug development.
- Build real-world evidence planning into Phase II. Registry design, patient-reported outcome selection, and post-market data collection strategies should be defined while clinical trial infrastructure is still active.
Translational judgment is the executive skill that ties these practices together. It requires interpreting scientific data across clinical and operational realities to make decisions that hold up under regulatory scrutiny, payer review, and real-world use. No platform or process substitutes for teams that have developed this judgment through experience.
Key takeaways
Translational medicine in biotech succeeds when preclinical evidence, medical affairs strategy, and advanced platforms are integrated from day one around explicit clinical decision gates.
| Point | Details |
|---|---|
| Define decision gates early | Assign each dataset a specific regulatory or clinical question before study design begins. |
| Validate biomarkers across species | Select biomarkers with measurable human analogs and prior clinical correlation before IND-enabling studies. |
| Embed Medical Affairs at IND stage | TMA involvement during protocol design prevents costly evidence gaps at payer and regulatory review. |
| Adopt platforms with fit-for-context specs | Organs-on-chips and AI tools require standardized measurement plans to generate decision-ready data. |
| Address the valley of death structurally | Cross-functional teams and proof-of-concept funding mechanisms, not scientific excellence alone, bridge academia to clinic. |
Why translational judgment is the skill biotech undervalues most
I have watched technically excellent programs fail not because the science was wrong, but because no one on the team could translate it. The data was real. The mechanism was sound. But the team could not articulate what the data meant for a Phase II patient population, a payer formulary committee, or a regulatory reviewer who had seen a hundred similar packages.
Translational judgment is not a soft skill. It is the ability to read a preclinical dataset and immediately ask: does this answer the clinical question, or does it answer a proxy for it? Most biotech teams are trained to generate data. Very few are trained to interrogate whether the data they are generating is the data that matters.
The platforms covered in this article, from organs-on-chips to TrialMatchAI, are genuinely useful. But they are tools. The teams that get the most from them are the ones who defined the clinical question before they turned the platform on. I have seen AI-driven multi-omics analyses produce beautiful visualizations that could not support a single IND decision because no one had specified what the output needed to demonstrate.
The most durable translational programs I have observed share one characteristic: they treat the patient outcome as the design constraint, not the hoped-for result. Every assay, every model, every platform choice flows backward from a specific clinical question about a specific patient population. That discipline is harder to build than any technology stack, and it is the one thing that cannot be outsourced.
— Hooman
How Innovabiotech supports your translational research pipeline
Translational medicine strategies depend on the quality of the molecular tools underlying them. Innovabiotech provides specialized peptide design and optimization services built for biotech teams that need precision at the molecular level to support IND-enabling and early clinical work. From de novo peptide design to protein engineering and enzyme optimization, Innovabiotech's San Francisco-based team works directly with your scientists to generate decision-ready data aligned with your translational milestones.
Whether your program requires hit-to-lead optimization, virtual screening, or high-throughput discovery support, Innovabiotech delivers customized solutions with full scientific transparency at every stage. Explore Innovabiotech's biotech advancements blog to see how these capabilities integrate with translational workflows across therapeutic areas.
FAQ
What is translational medicine in biotech?
Translational medicine is the systematic process of converting laboratory discoveries into clinical therapies by aligning preclinical evidence, clinical trial design, and real-world outcomes. In biotech, it functions as the decision-making framework that determines which compounds advance and how.
How does biotechnology influence healthcare through translational medicine?
Biotechnology accelerates healthcare impact by providing the molecular tools, biomarker platforms, and data-driven models that translational medicine requires to move compounds from bench to patient. NCATS at NIH identifies improved patient-response models and real-world data integration as the primary mechanisms driving this acceleration.
What is the valley of death in translational research?
The valley of death describes the funding and infrastructure gap between academic discovery and clinic-ready product development. Translational core facilities, SBIR/STTR grants, and cross-functional teams with regulatory expertise are the primary mechanisms for bridging it.
How do organs-on-chips improve translational drug development?
Organs-on-chips provide reproducible human physiology models that benchmark quantitatively against clinical pharmacokinetics and toxicology data, improving the predictive accuracy of preclinical decisions. Regulatory acceptance requires standardized measurement plans linking chip readouts directly to clinical data.
Why should Medical Affairs be embedded early in biotech development?
Early TMA embedding allows payer evidence needs and regulatory alignment to be built into clinical trial design before the protocol is finalized. This prevents the evidence gaps that are expensive or impossible to close after Phase III data is locked.