TL;DR:
- Patient stratification in biotech involves dividing patients into molecular subgroups using multi-omics data to improve treatment outcomes. It relies on integrating biomarkers and clinical information into workflows that guide personalized therapy and enhance clinical trial design. Challenges include ensuring data harmonization, model interpretability, and embedding stratification into clinical practice effectively.
Patient stratification in biotech is defined as the process of dividing patients into molecularly and clinically distinct subgroups to predict prognosis, optimize treatment selection, and improve clinical trial outcomes. This methodology uses multi-omics profiles including genomic, transcriptomic, proteomic, and metabolomic data layers to identify which patients will respond to a given therapy. In drug development, stratification is the difference between a trial that demonstrates efficacy and one that fails at phase III. AI platforms, biomarker panels, and computational frameworks have made it possible to process these complex data sets at scale, turning what was once a manual clinical judgment into a reproducible, data-driven workflow.
What is patient stratification in biotech?
Patient stratification is the formal methodology of segmenting a patient population into subgroups based on shared molecular, clinical, or phenotypic characteristics. The goal is precision: matching the right therapy to the right patient at the right dose. This is the operational foundation of personalized medicine.

The process draws on several data types simultaneously. Genomic sequencing identifies mutations and copy number variations. Transcriptomic profiling reveals gene expression patterns. Proteomic and metabolomic analyses capture downstream biological activity. Integrating these layers gives researchers a far more complete picture of disease biology than any single data type can provide.
Biomarkers are the currency of stratification. A biomarker is any measurable biological indicator, such as a protein level, gene variant, or microbial signature, that correlates with disease state or treatment response. In oncology, HER2 expression stratifies breast cancer patients for trastuzumab therapy. In immunotherapy, PD-L1 expression predicts checkpoint inhibitor response. These are not theoretical constructs. They are clinically validated decision points that determine who receives which treatment.
The importance of patient stratification extends beyond treatment selection. In clinical trials, stratification defines enrollment criteria, controls for confounding variables, and increases the statistical power of efficacy analyses. A trial that enrolls a biologically homogeneous subgroup needs fewer patients to detect a treatment effect. That translates directly into faster timelines and lower development costs.
How does patient stratification work in practice?
The methodology behind biotech patient stratification combines molecular profiling, computational analysis, and clinical data integration into a structured workflow.
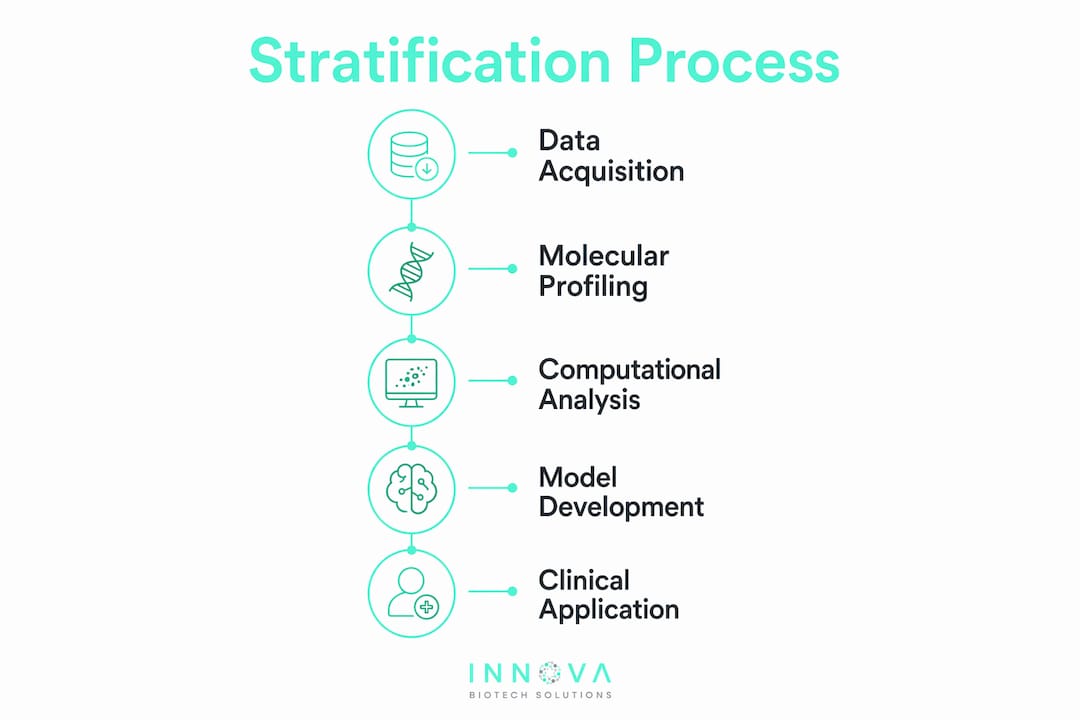
Data acquisition is the starting point. Researchers collect biological samples, electronic health records, imaging data, and patient-reported outcomes. The richer the data set, the more granular the subgroup identification.
Multi-omics integration is where the complexity lies. Each omics layer captures a different dimension of biology. Genomics tells you what could happen. Transcriptomics tells you what is happening. Proteomics and metabolomics tell you what the cell is actually doing. Combining these layers identifies precise disease subgroups that single-layer analysis would miss entirely.
AI and machine learning process the volume and dimensionality of multi-omics data that no manual analysis can handle. Algorithms identify patterns across thousands of variables simultaneously, flagging subpopulations with distinct biological signatures. However, AI-driven stratification faces real implementation hurdles, including algorithm interpretability, data harmonization across institutions, and ethical considerations around data use. These are not minor technical footnotes. They are the primary barriers to clinical adoption.
Subgroup assignment translates computational outputs into actionable patient categories. In risk-based models, patients are typically grouped into 3–5 tiers based on clinical complexity and projected resource needs. Each tier maps to a specific care protocol, visit frequency, or treatment pathway.
- Genomic biomarkers: mutation status, copy number variation, microsatellite instability
- Transcriptomic markers: gene expression signatures, RNA splicing variants
- Proteomic markers: circulating protein levels, post-translational modifications
- Microbial biomarkers: gut microbiome composition linked to immunotherapy response
- Clinical markers: imaging findings, lab values, comorbidity scores
Pro Tip: When building a stratification pipeline, prioritize data harmonization before model development. Inconsistent units, missing values, and platform-specific batch effects will corrupt downstream subgroup assignments regardless of how sophisticated your algorithm is. Establish a data governance protocol at the project outset.
Which stratification methods work best for biotech research?
Biotech patient stratification methods fall into three broad categories, each with distinct strengths, data requirements, and clinical use cases.
| Method | Data Inputs | Strengths | Limitations | Best Use Case |
|---|---|---|---|---|
| Rule-based | Clinical thresholds, lab values | Transparent, auditable, easy to implement | Misses complex interactions | Primary care risk tiers, formulary decisions |
| Predictive (ML/AI) | Multi-omics, EHR, imaging | Handles high-dimensional data, finds non-linear patterns | Low interpretability, needs large training sets | Oncology subtyping, drug response prediction |
| Hybrid | Clinical rules + predictive scores | Balances transparency and accuracy | Complex to validate and maintain | Trial enrollment, precision dosing |
Rule-based approaches offer transparency that clinicians and regulators can audit. A patient with an HbA1c above a defined threshold falls into a specific management tier. The logic is visible. Predictive models, by contrast, identify subgroups that no clinician would have defined manually. They find the signal in noise that human pattern recognition cannot detect.
Hybrid models are increasingly the standard in serious drug development programs. They combine the clinical credibility of rule-based criteria with the pattern-detection power of machine learning. Multi-objective synergy models represent a further refinement, quantifying inter-individual variability to optimize combination therapy dosing per subgroup. Voxel-based stratification within these frameworks identifies subpopulations that lack meaningful response to a given drug combination, preventing unnecessary exposure.
The practical challenge is biomarker availability. Not every patient arrives with a complete molecular profile. Initiation protocols address this by defining the minimum parameter set needed to assign a patient to a subgroup before full therapy begins. This is a critical design consideration for any stratification system deployed in a real clinical setting.
How does stratification improve drug development and clinical trials?
The clinical applications of patient stratification in healthcare span oncology, neurology, immunology, and rare disease, with the most mature examples in cancer drug development.
In oncology, stratification by PD-L1 expression, tumor mutational burden, and microsatellite instability status has transformed immunotherapy trial design. Trials that enroll unselected populations often fail to show efficacy because responders are diluted by non-responders. Stratified enrollment concentrates the signal.
In Alzheimer's disease research, stratified cohorts by risk level show significantly different hazard ratios for clinical outcomes such as nursing home admission (HR 0.804, 95% CI 0.765–0.844 for lower-risk groups). That magnitude of difference in outcome trajectory means a trial that ignores stratification is essentially measuring noise.
Companion diagnostics (CDx) are the regulatory and operational bridge between stratification science and trial execution. A CDx test identifies which patients qualify for a specific therapy based on a defined biomarker. Early alignment of CDx tests with trial inclusion criteria is the single most important step in avoiding enrollment inefficiencies and missed efficacy endpoints. Misalignment between the diagnostic and the endpoint is a common and expensive failure mode.
Operationalizing stratification in clinical workflows requires more than a scoring algorithm. Tier-based visit protocols and care team assignments are what convert a stratification output into a patient outcome. The data science is only as valuable as the clinical process it feeds.
- Stratification reduces trial sample size requirements by increasing biological homogeneity within arms
- CDx alignment with inclusion criteria prevents enrollment of non-responders
- Risk-tiered care protocols direct high-complexity patients to specialist teams
- Stratification outputs must map to specific clinical actions, not just risk scores
Pro Tip: Define your stratification endpoints before you select your biomarkers. Working backward from the clinical decision you need to make forces you to choose biomarkers that are actually actionable, rather than biomarkers that are merely measurable.
What are the biggest challenges in ai-driven patient stratification?
The future of biotech patient stratification runs through AI, but the path has real obstacles that researchers need to plan around rather than assume away.
Data harmonization is the most pervasive problem. Multi-site studies generate data on different platforms, with different preprocessing pipelines and different missing data patterns. An algorithm trained on one institution's data often fails to generalize to another's. Federated learning approaches are emerging as a partial solution, allowing models to train across distributed data sets without centralizing sensitive patient information.
Algorithm interpretability is a regulatory and clinical trust issue. A black-box model that assigns patients to treatment arms without explainable logic will not pass regulatory scrutiny and will not earn clinician adoption. Topology-informed graph frameworks like PathTIGR address this by embedding biological pathway relationships directly into the model architecture. The result is a model that predicts and explains, connecting genomic inputs to known mechanistic pathways.
Ethical considerations around genomic data use, consent, and algorithmic bias are not peripheral concerns. Stratification algorithms trained on non-representative populations will systematically misclassify underrepresented groups. This is a scientific problem as much as an ethical one.
- Standardize data collection protocols across all contributing sites before model development begins
- Select interpretable model architectures or build post-hoc explanation layers for complex models
- Audit training data for demographic representation and correct for known biases
- Validate stratification outputs prospectively in independent cohorts before clinical deployment
- Integrate stratification outputs directly into electronic health record workflows to drive clinical action
Digital twin platforms represent the next frontier. A digital twin is a computational model of an individual patient that simulates biological responses to different interventions. Combined with real-time biomarker monitoring, digital twins could enable dynamic stratification that updates as a patient's biology changes during treatment. The translational medicine pipeline connecting these computational models to clinical practice is still maturing, but the trajectory is clear.
Key takeaways
Patient stratification is effective only when molecular subgroup assignments are directly connected to clinical decisions, trial endpoints, and care protocols.
| Point | Details |
|---|---|
| Multi-omics is the foundation | Integrating genomic, transcriptomic, proteomic, and metabolomic data identifies subgroups single-layer analysis misses. |
| Method selection drives outcomes | Rule-based models offer transparency; predictive models handle complexity; hybrid models suit most drug development programs. |
| CDx alignment is non-negotiable | Companion diagnostics must align with trial inclusion criteria early to prevent enrollment failures and missed endpoints. |
| AI needs interpretability | Topology-informed models like PathTIGR improve both prediction accuracy and mechanistic explainability for clinical adoption. |
| Operationalization determines impact | Stratification outputs must connect to tiered care protocols and clinical workflows to generate real patient outcomes. |
Stratification is a clinical workflow, not a data project
The framing I see most often in research proposals treats patient stratification as a computational problem. Build the model, validate the subgroups, publish the paper. That framing misses the point entirely.
Stratification is only valuable when it changes what a clinician does next. A risk score that sits in a database and never triggers a care team assignment, a modified visit schedule, or a treatment decision has zero clinical impact. The operational embedding of stratification into daily clinical workflows is where most programs fail, and it is almost never a data science problem. It is a process design and change management problem.
The biomarker strategy question is equally underappreciated. Researchers often select biomarkers based on what is measurable rather than what is actionable. A biomarker that stratifies patients beautifully in a retrospective analysis but cannot be measured in a standard clinical lab within a clinically relevant timeframe is not a useful stratification tool. Actionability has to be built into the biomarker selection criteria from day one.
The programs I find most credible are the ones that start with the clinical decision and work backward. What action will change based on this patient's subgroup assignment? What is the minimum biomarker set needed to make that assignment reliably? What is the turnaround time requirement? Those questions force a discipline that purely data-driven approaches rarely impose on themselves.
The field is moving fast. AI is genuinely expanding what is possible. But the fundamentals have not changed. Stratification that does not connect to clinical action is an academic exercise.
— Hooman
How Innovabiotech supports precision stratification research
Biomarker discovery and computational validation are where stratification programs succeed or stall. Innovabiotech brings both capabilities to research teams that need to move from molecular hypothesis to clinically deployable subgroup model.
Innovabiotech's peptide design and bioinformatics services support biomarker development, companion diagnostic validation, and therapeutic candidate optimization for stratified patient populations. The team works across virtual screening, protein engineering, and de novo peptide design, giving researchers the computational and experimental depth needed to build stratification-ready molecular tools. If your program needs to connect multi-omics data to a specific clinical decision point, Innovabiotech's protein design services provide the structural and functional modeling to get there. Reach out to discuss your stratification project.
FAQ
What is patient stratification in biotech?
Patient stratification in biotech is the process of dividing patients into molecularly defined subgroups using multi-omics data, biomarkers, and clinical variables to predict treatment response and optimize therapy selection. It is the operational foundation of precision medicine and clinical trial design.
How does patient stratification work in clinical trials?
Stratification defines enrollment criteria based on validated biomarkers, ensuring trial arms contain biologically similar patients. This increases statistical power and reduces the sample size needed to detect a treatment effect.
What are the main biotech patient stratification methods?
The three primary methods are rule-based models, predictive machine learning models, and hybrid models. Rule-based approaches offer transparency; predictive models handle high-dimensional multi-omics data; hybrid models combine both for complex drug development programs.
Why does companion diagnostic alignment matter for stratification?
Misalignment between companion diagnostics and trial endpoints causes enrollment of non-responding patients, which dilutes efficacy signals and increases trial failure risk. Early CDx alignment with inclusion criteria is the most direct way to protect trial integrity.
What is the biggest challenge in ai-driven patient stratification?
Algorithm interpretability and data harmonization across institutions are the primary barriers to clinical adoption. Topology-informed frameworks like PathTIGR address interpretability by embedding biological pathway knowledge directly into model architecture.