TL;DR:
- The peptide therapeutic development process involves target identification, design, synthesis, formulation, safety testing, and manufacturing. The market for peptide therapeutics is expected to exceed $250 billion by 2030, reflecting their growing importance in drug discovery. Successful programs depend on early integration of design, formulation, regulatory planning, and collaboration across disciplines to avoid late-stage failures.
The peptide therapeutic development process is defined as the coordinated sequence of target identification, computational design, chemical synthesis, formulation, preclinical safety testing, and GMP manufacturing required to advance a peptide from concept to clinical candidate. The global peptide therapeutics market is projected to exceed $250 billion by 2030, driven by a compound annual growth rate above 9% across metabolic, oncology, and immunological indications. That scale reflects how central peptides have become to modern drug discovery. This guide walks biotech professionals through every phase of the pipeline, covering AI-driven peptide drug design, synthesis methods, formulation strategies, regulatory frameworks, and the transition to scalable manufacturing.
What are the essential stages of the peptide therapeutic development process?
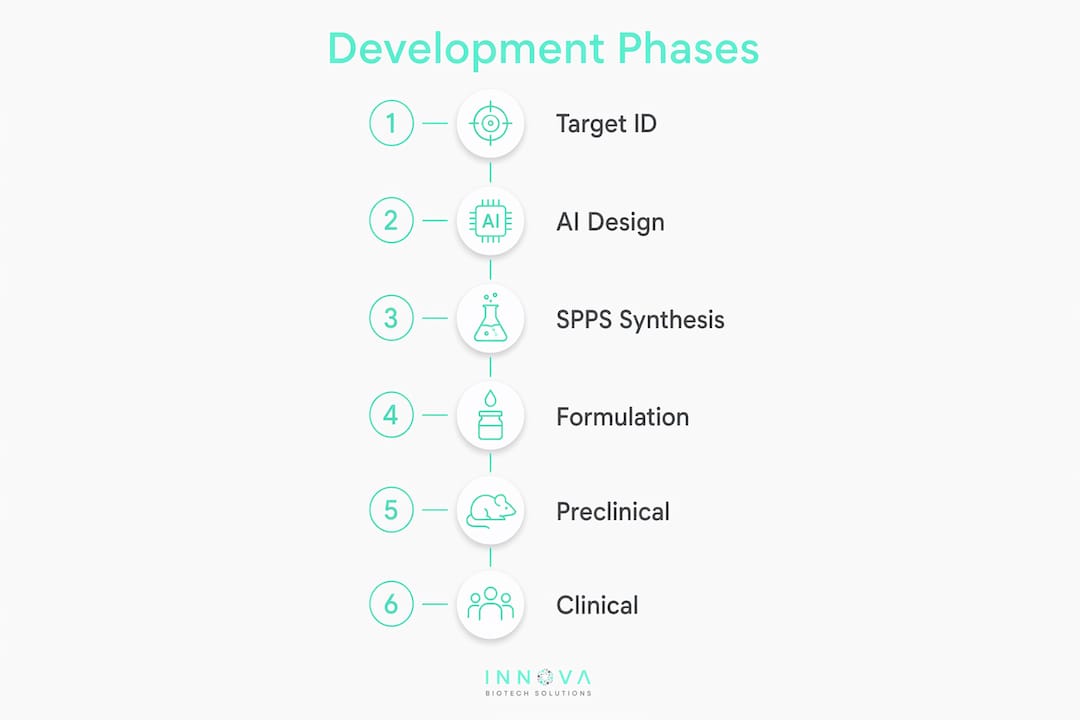
The six-phase development workflow spans target identification, AI-assisted design, solid-phase peptide synthesis (SPPS), formulation development, preclinical testing, and GMP manufacturing. Each phase has defined objectives, and failure to meet them creates downstream attrition. Contract development and manufacturing organizations (CDMOs) are now embedded in most commercial programs, providing synthesis capacity, analytical services, and regulatory support across multiple phases.
The table below maps each phase to its primary tools and objectives:
| Phase | Primary Tools | Objective |
|---|---|---|
| Target Identification | Bioinformatics, proteomics, structural biology | Validate druggable target and binding site |
| AI-Assisted Design | Machine learning, generative models, docking | Generate and rank candidate sequences |
| SPPS Synthesis | Fmoc/tBu chemistry, automated synthesizers | Produce high-purity peptide for testing |
| Formulation Development | PEGylation, lipidation, cyclization, CPPs | Improve stability, delivery, and pharmacokinetics |
| Preclinical Testing | In vitro assays, rodent and primate models | Establish safety, efficacy, and PK profile |
| GMP Manufacturing | Validated processes, QC systems, CDMOs | Scale production for IND filing and clinical supply |
Early coordination between discovery, process development, and manufacturing is critical to reduce late-stage attrition and maintain a path to scalable, compliant production. Programs that treat manufacturing as a phase-six concern routinely face costly redesigns. Building manufacturability criteria into the design phase is not optional at a commercial scale.
How does ai-driven peptide design enhance therapeutic development?
AI accelerates therapeutic peptides development by compressing the sequence generation and optimization cycle from months to days. Machine learning models trained on structural and activity databases can propose novel sequences, predict binding affinity, and flag liabilities such as aggregation or protease sensitivity before any synthesis occurs. Generative models including variational autoencoders and diffusion-based architectures now produce peptide libraries with defined physicochemical constraints.
The practical limits of AI in peptide drug design are equally important to understand:
- Binding affinity prediction from AI models correlates with experimental data but does not replace it. Physics-based scoring functions remain necessary for final candidate selection.
- Generative models produce sequences that are chemically plausible but not always synthetically accessible or metabolically stable.
- Immunogenicity prediction tools like NetMHCpan provide useful signals, but wet-lab confirmation is mandatory before advancing to in vivo studies.
- Formulation compatibility is rarely captured by current AI models, meaning a computationally optimized sequence may still fail in a physiologically relevant delivery system.
AI-generated peptide sequences require rigorous physics-based binding energy screening and bench validation, confirming that in silico design is hypothesis-driven rather than conclusive. This framing matters operationally. Teams that treat AI outputs as final candidates waste synthesis resources and delay programs. Teams that treat them as ranked hypotheses move faster.
Pro Tip: Pair AI-generated candidate lists with binding affinity prediction workflows that apply molecular dynamics or MM-GBSA rescoring before committing to synthesis. This step filters out false positives that pass initial docking screens.
Despite advances in AI, peptide development demands interdisciplinary expertise that integrates computational predictions with medicinal chemistry and formulation science. No single discipline owns the outcome.
What challenges and regulatory considerations must be addressed?
Proteolytic degradation is the primary stability challenge in therapeutic peptides development. Linear peptides are rapidly cleaved by serum and gastrointestinal proteases, limiting half-life and oral bioavailability. Oral delivery remains particularly difficult. Semaglutide's oral formulation, co-developed with the absorption enhancer SNAC, required years of concurrent molecular and formulation optimization to achieve clinically meaningful bioavailability. That example is now the benchmark for what integrated design-delivery looks like in practice.
Regulatory alignment must begin at the design stage, not at the IND submission. The key ICH guidelines governing peptide programs are:
- ICH M3(R2): Defines nonclinical safety study timing relative to clinical trial phases.
- ICH S6(R1): Addresses safety testing for biotechnology-derived pharmaceuticals, including peptides with biological activity.
- ICH Q8 through Q12: Covers pharmaceutical development, quality risk management, and lifecycle management of drug substances and products.
Noncompliance with ICH guidelines causes regulatory delays that can set programs back by 12–24 months. The cost is not just time. Late-stage regulatory deficiencies often require additional studies that were avoidable with earlier planning.
Regulatory agencies differ in their application of ICH guidelines, which makes early and extensive characterization of immunogenicity and impurities necessary for multi-region approvals. The FDA, EMA, and PMDA each interpret immunogenicity risk thresholds differently. Programs targeting global markets need a characterization package that satisfies the most stringent agency from the start.
Early multidisciplinary coordination between regulatory affairs, formulation science, and clinical pharmacology is the single most effective way to prevent late-stage program failure in peptide therapeutics.
What are best practices for peptide synthesis and formulation?
Solid-Phase Peptide Synthesis (SPPS) is the primary method for precise peptide assembly, preferred for its reproducibility across research and commercial manufacturing. SPPS uses Fmoc or Boc chemistry to build sequences one amino acid at a time on a solid resin support, allowing precise control over sequence fidelity and enabling the incorporation of non-natural amino acids. Liquid-Phase Peptide Synthesis (LPPS) remains relevant for shorter sequences and specific industrial applications where cost efficiency outweighs the flexibility advantages of SPPS.
The comparison below summarizes the key differences:
| Attribute | SPPS | LPPS |
|---|---|---|
| Sequence length | Up to 50+ residues | Best for 2–10 residues |
| Scalability | High, with automation | Moderate |
| Non-natural amino acids | Readily incorporated | Limited |
| Purification complexity | Moderate to high | Lower |
| Cost at scale | Higher per gram | Lower for short sequences |
Formulation strategy directly determines whether a synthesized peptide reaches its target intact. Key formulation methods include PEGylation, lipidation, cyclization, and cell-penetrating peptides (CPPs), each addressing different stability and delivery challenges. PEGylation extends half-life by reducing renal clearance and protease access. Lipidation, as used in semaglutide and liraglutide, enables albumin binding and prolonged circulation. Cyclization constrains peptide conformation, improving both receptor selectivity and proteolytic resistance.
Pro Tip: Evaluate stapled peptide design as a formulation-adjacent strategy for intracellular targets. Hydrocarbon stapling locks alpha-helical conformation, dramatically improving cell penetration and metabolic stability without requiring a separate delivery vehicle.
Modern successful peptide projects integrate formulation and delivery strategies such as lipid conjugation and permeation enhancers at the design outset. Waiting until synthesis is complete to consider delivery is a structural program risk.
How to manage preclinical safety testing and move to clinical manufacturing
Preclinical safety testing for peptide candidates follows a defined sequence before any first-in-human study. Nonclinical safety assessment must include repeated-dose toxicity, toxicokinetics, safety pharmacology, and genetic toxicology, with species selected to reflect human metabolism and target engagement.
The standard preclinical progression looks like this:
- In vitro safety profiling: hERG channel assays, cytotoxicity panels, and plasma stability testing establish early liability flags.
- Rodent toxicology: Rat studies provide dose-range finding data and initial toxicokinetic profiles.
- Non-rodent toxicology: Cynomolgus monkey or minipig studies are required when the peptide shows pharmacological activity in a second species relevant to the human target.
- Safety pharmacology: Cardiovascular, respiratory, and CNS assessments per ICH S7A and S7B guidelines.
- Genetic toxicology: Ames test and in vitro micronucleus assay are standard; in vivo studies follow if signals emerge.
Peptides follow classical pharmacokinetics with predictable allometric scaling, which means nonclinical PK data can reliably forecast human exposure when species are selected correctly. This predictability is a genuine advantage over large biologics, where allometric scaling is less reliable. Programs that invest in early pharmacokinetic modeling reduce the risk of dose selection errors in Phase 1 clinical trials for peptides.
GMP manufacturing readiness is the final gate before IND filing. CDMOs with peptide-specific GMP infrastructure provide validated synthesis processes, analytical method packages, and batch records that meet FDA and EMA expectations. The decision to transfer synthesis to a CDMO should occur no later than the end of preclinical development, allowing sufficient time for process characterization and scale-up validation before clinical supply is needed.
Key takeaways
The peptide therapeutic development process succeeds when target identification, AI-assisted design, synthesis, formulation, preclinical safety, and GMP manufacturing are integrated from day one rather than treated as sequential handoffs.
| Point | Details |
|---|---|
| Integrate design and delivery early | Concurrent formulation planning at the design stage reduces late-stage attrition and bioavailability failures. |
| Use AI as a hypothesis generator | AI-designed sequences require physics-based rescoring and bench validation before synthesis commitment. |
| Align with ICH guidelines from the start | ICH M3(R2), S6(R1), and Q8–Q12 compliance must be built into the development plan, not retrofitted. |
| Select synthesis method by peptide properties | SPPS is preferred for sequences above 10 residues and programs requiring non-natural amino acid incorporation. |
| Engage CDMOs before IND filing | Early CDMO involvement allows process characterization and scale-up validation before clinical supply timelines become critical. |
Where i think most peptide programs go wrong
The delivery problem nobody wants to own
After working across multiple peptide programs, the pattern I see most often is not a design failure. It is a delivery failure that was predictable from sequence selection. Teams fall in love with a binding profile, advance through synthesis, and then discover that the peptide degrades in serum within minutes or cannot cross the relevant biological barrier. The formulation team inherits a problem that was baked in at the design stage.
The shift to concurrent design-delivery optimization is the most important structural change a peptide program can make. Oral semaglutide is the clearest proof point. That molecule required co-optimization of the peptide structure, the fatty acid conjugate, and the SNAC absorption enhancer simultaneously. None of those elements worked in isolation.
My second observation is about AI. The field has overcorrected toward treating generative model outputs as near-final candidates. I have seen programs burn three to four synthesis cycles on AI-proposed sequences that failed basic plasma stability screens. The fix is not to abandon AI. The fix is to treat every AI output as a ranked hypothesis and apply de novo design principles alongside experimental triage before committing resources.
The programs that move fastest are the ones where regulatory affairs, formulation science, and computational chemistry are in the same room from the first design review. That integration is harder to build than any individual technical capability, but it is what separates programs that reach the clinic from programs that stall in late preclinical.
— Hooman
How Innovabiotech supports your peptide development program
Innovabiotech provides end-to-end support for teams advancing peptide candidates through discovery, optimization, and manufacturing readiness. The San Francisco-based team combines AI-driven sequence generation, bioinformatics validation, and medicinal chemistry expertise to move candidates from target to optimized lead faster than traditional sequential workflows allow.
Whether you need custom peptide design services for a de novo program or computational support to rescue a stalled candidate, Innovabiotech's team works directly with your scientists at every stage. Services cover virtual screening, hit-to-lead optimization, and GMP-ready process development. For programs requiring protein engineering alongside peptide work, the protein design services team provides complementary computational modeling and structural analysis. Contact Innovabiotech to discuss your program's current stage and where expert support can accelerate your path to the clinic.
FAQ
What are the six phases of peptide therapeutic development?
The six phases are target identification, AI-assisted design, SPPS synthesis, formulation development, preclinical safety testing, and GMP manufacturing. Each phase has defined deliverables that gate progression to the next stage.
How does SPPS differ from liquid-phase synthesis for therapeutic peptides?
SPPS is preferred for sequences above 10 residues and programs requiring non-natural amino acids, offering higher reproducibility and automation compatibility. LPPS is more cost-efficient for short sequences but offers less flexibility for complex modifications.
Which ICH guidelines apply to peptide drug development?
ICH M3(R2), S6(R1), and Q8 through Q12 are the primary guidelines governing nonclinical safety, biotechnology-derived drug safety, and pharmaceutical quality for peptide programs. Noncompliance with these guidelines is a leading cause of regulatory delays.
What preclinical tests are required before clinical trials for peptides?
Repeated-dose toxicity, toxicokinetics, safety pharmacology, and genetic toxicology studies are required, with species selected to reflect human target engagement and metabolism. Peptides follow predictable allometric scaling, making nonclinical PK data a reliable basis for human dose selection.
When should a peptide program engage a CDMO?
CDMO engagement should occur no later than the end of preclinical development to allow sufficient time for process characterization, analytical method transfer, and GMP batch production before clinical supply timelines become critical.
Recommended
- Bioinformatics Peptide Optimization: A 2026 Guide for Pharma
- Protein Engineering for Therapeutics: A 2026 Guide
- De Novo Peptide Design Benefits for Drug Discovery
- Innova Biotech Solutions: Expert Peptide Design and Optimization Services.bioinformatics validation, custom peptides, peptide design services